

Business Spectator’s Callam Pickering has written another good post questioning the Commission of Audit’s (COA) recommendations that: 1) higher income earners take-out private health insurance for basic health services (instead of Medicare); and 2) introducing a $15 co-payment for all Medicare funded services (up to 15 services) and $7.50 per service thereafter, with concession card holders paying $5 per service (up to 15 services) and $2.50 thereafter:
The commission’s plan to direct Australians – rich or otherwise – towards private health insurance… effectively… substitutes private spending on health for public spending. The issue is that private health insurance is typically more expensive than its public equivalent because the government is better placed to use its market power to lower costs and is better able to manage insurance risks.
If we think about the total health sector (public and private spending), higher spending on private health insurance would actually leave Australians worse off, with fewer services per dollar spent. Effectively our health burden would increase.
Instead of forcing high income earners to take out private health insurance, the government would be better off directing those funds to public health spending via a higher tax or Medicare levy…
Co-payments are easier to justify and are actually a fairly good idea. A small payment can be an effective method to manage demand for health services and emergency departments… [But]… the system suggested by the commission is likely to place a greater burden on concession holder… Personally I’d prefer a system that based your co-payments on your capacity to pay rather than a fixed two-tier system.
Private health insurance may reduce the level of public health spending but is likely to increase total health spending across the economy. Reducing health costs is important but the government should place greater emphasis on improving productivity and identifying the most effective procedures rather than passing the responsibility on to someone else.
The COA’s focus on Medicare is justified given the 124% escalation in Medicare Benefits Scheme (MBS) outlays (from $8.1 billion to $18.6 billion) between 2002-03 and 2012-13, as well as the projected increase in health care spending as Australia’s population ages (see next chart).
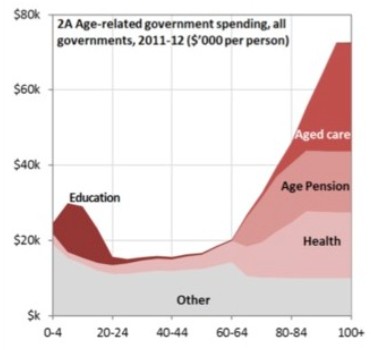
In its 2010 Intergenerational Report, Treasury projected that Commonwealth health expenditure would balloon from 4% of GDP to 7% of GDP by 2050 without policy change, just as the taxation base shrinks due to an ageing population. So health costs will either need to be paired-back or taxes will need to rise significantly.
In principle, I agree with Pickering that introducing a small co-payment for Medicare services is a sensible move, provided there are adequate safeguards for lower income earners and the poor.
Medicare co-payments can work as an important demand management tool. Without some kind of out-of-pocket expense, GP and associated Medicare services are likely to be overused, without due regard given to the overall cost to taxpayers and the Budget. Better price signals are, therefore, required in order to better ration services – as occurs with other government health services, such as existing payments to a pharmacist for prescriptions.
Of course, there should always be safeguards for vulnerable citizens, such as those on health care cards or on very low incomes, and I would prefer to see “free” (or close to free) Medicare services reserved only for these cohorts. But that does not mean that the majority of people with adequate means should not pay something when they consume public health services.
However, the COA’s plan to shift GP costs onto private health insurers is far more contentious, and would likely lead to an escalation in private health insurance premiums. While such a reform may lower direct costs to the Budget, overall health costs to the economy (and households) could rise significantly, making the community worse-off as a whole.
Indeed, the US health system illustrates the perils of moving towards a privatised system. There, healthcare consumes 18% of GDP, versus 9% in Australia, despite 16% of US households not being covered by any form of health insurance and much worse overall health outcomes.
A recent survey by Bloomberg ranking countries based on three criteria: life expectancy; relative per capita cost of health care (percentage of GDP per capita); and the absolute per capita cost of health care, also showed Australia to have the 7th most efficient health care system in the world, ranking above other Anglosphere nations including the UK (14th), Canada (17th) and the United States (46th).
While better price signals are certainly required in order to better ration services, the Government should be very wary about making fundamental changes to the system, including shifting health provision to private operators.
Finally, Pickering also notes that the Government should focus on achieving greater health service efficiency by identifying and using the most cost-effective, evidenced-based procedures.
Again, this is a sound approach and certainly would do more to hold down the nation’s overall health costs than taking the lazy approach of ‘passing the buck’ to more expensive private operators.
unconventionaleconomist@hotmail.com
