Back in June, Mike Moynihan and Bob Birrell from the Australian Population Research Institute released a report showing that the number of doctors has easily out-paced growth in the population, driven largely by a conga-line of OTDs that enter Australia to work in a regional area only to then move to the already-oversupplied city once their mandatory term is up.
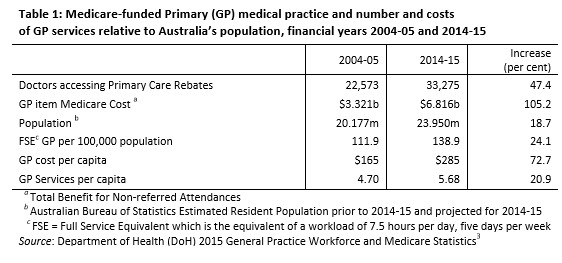
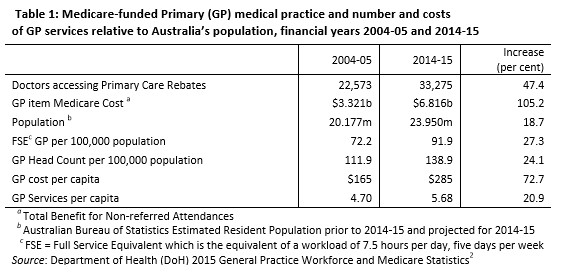
According to this research, the number of doctors in Australia rose by 47% in the decade to 2014-15, around 2.5 times the 19% growth in the overall population:
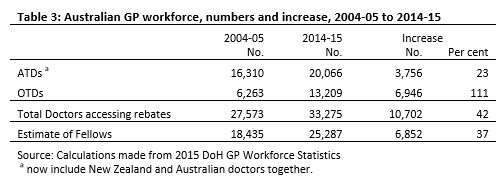
Much of this growth has come from OTDs, whose numbers have ballooned-out by a whopping 111% over this period. Most of these doctors are also practicing in over-supplied metropolitan areas, not areas of shortage:
Advertisement
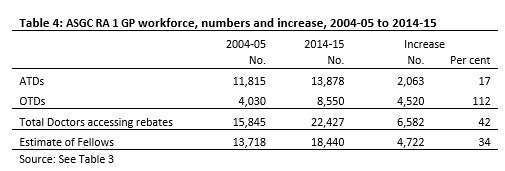
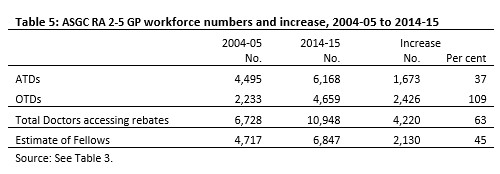
The purpose of the OTD promotion policy was to get more doctors into underserviced areas, particularly RA 2-5 areas. But Tables 4 and 5 show that most of the extra OTDs, by 2014-15, were practising in RA 1 areas.5 Of the total increase in OTDs (6,946) shown in Table 3, 4,520 were practising in RA 1 areas and 2,426 in RA 2-5 areas.
What has happened is that there has been a gradual leaching of OTDs into RA 1 areas where there is an ample supply of doctors, as well as into the more attractive provincial cities such as Ballarat, Bendigo and Shepparton in Victoria, where the situation is similar…
The report also noted that OTDs are not only responsible for much of the doctor oversupply, but also the blow-out in Medicare rebates:
Advertisement
The OTDs influx is therefore responsible for most of the growing oversupply of GPs in RA 1 locations. They are also responsible for most of the increase in Medicare service costs. By June 2015, for all of Australia, OTDs made up 39.7 per cent of the workforce but received 49.8 per cent of total rebates. In RA 1 areas they made up 38.1 per cent of the total workforce and received 47.6 per cent of services paid for by Medicare.
The consequences of which are a continued blow-out in bulk-billed GP visits and Medicare funding costs.
Now, Moynihan and Birrell have released a follow-up report entitled GP Oversupply – Ignoring the Evidence, which examines the issue in further detail. Below is the report summary:
Advertisement
The Coalition has tried to curb the costs of GP non-referred attendances. The charge to the taxpayer has grown from $3.3 billion in 2004-05 to $6.8 billion in 2014-15 (Table 1) and $7.2 billion in 201516. This is just one of many expenditure blowouts the Coalition has failed to control.
The one measure implemented, first by the Labor Government then extended to 2020 by the Coalition Government, was to put a cap on Medicare rebates paid for GP services. The hope was that this would slow the growth in the public bill for providing GP services. This measure has failed. Why?
The main reason is that the Coalition has presided over a surge in the number of GPs billing on Medicare, particularly in Australia’s metropolitan areas. The dominant source of these extra doctors is overseas-trained doctors (OTDs) who have completed their compulsory period of service in undersupplied locations.
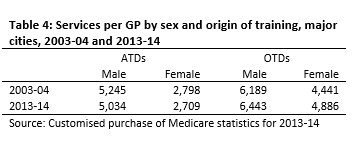
Most subsequently move to the major cities and regional centres. These OTDs are the main source of the rapid growth in the per capita provision of GP services in the cities. This is partly because of the surge in their numbers and partly because they bill for far more services per year than their Australian-trained doctor (ATD) counterparts (Table 4).
Meanwhile, in regional areas, the government is allowing employers to sponsor OTDs to replace those who have served their required time in areas defined as in shortage. Employers continue to sponsor more than 2,000 replacement OTDs on 457 visas each year (2,320 in 2015-16). This is more than the 1,529 training places for local graduates beginning their careers as GPs in 2015.
The result is a cycle leading to ever larger numbers of doctors relative to Australia’s patient load and ever higher GP Medicare costs.
GPs are being forced to chase patients. However, the competition has not stopped a continuing increase in Medicare services. This is because GPs can manage their patient load to generate extra services (as with repeat visits and tests). For their part, patients, though showing some evidence of resistance to multiple visits and the like, do not have to pay any extra costs. High throughput practices have to bulk-bill. Some 85 per cent of all GP services are now bulk-billed.
Over the next few years, the Coalition Government faces a further surge in GP numbers due to the doubling of Australian medical school graduate numbers since the mid-2000s. Its own Department of Health has proposed dealing with the oversupply by reducing medical migration and requiring Australian graduates to serve where they are needed.
The Coalition Government rejected this advice, partly because it was afraid of the opposition that organised medicine always mounts to such proposals.
As matters stand, GP costs will continue to mount. Worse, because so many GPs are now pursuing patients, increasing numbers of GPs are resorting to high throughput medicine in order to achieve their income targets. Medicare billing costs are rising yet the quality of medical care is diminishing.
Clearly, controlling Medicare costs requires more than just the elimination of wasteful practices, but also reining in the 457 visa rort that has oversupplied our cities with GPs.
The Australian Medical Association recently called for changes to Australia’s visa system to prevent the widespread importation of foreign trained medical staff. Let’s hope the Government takes action.
Leith van Onselen is Chief Economist at the MB Fund and MB Super. He is also a co-founder of MacroBusiness.
Leith has previously worked at the Australian Treasury, Victorian Treasury and Goldman Sachs.